

This is a transcript of an interview with Dr. Peter Goadsby. Teri and I had the privilege of meeting with him in San Francisco at the June 2018 AHS Scientific Meeting. In the interview, we discussed the recent results of the Autonomic Technologies clinical trial of their sphenopalatine ganglion microstimulator system. As a chronic Cluster Headache patient, I was excited to hear his perspective on the trial results and what it might mean for patients like me.
Tammy Rome:
What do patients need to know about SPG neurostimulation?
Dr. Goadsby:
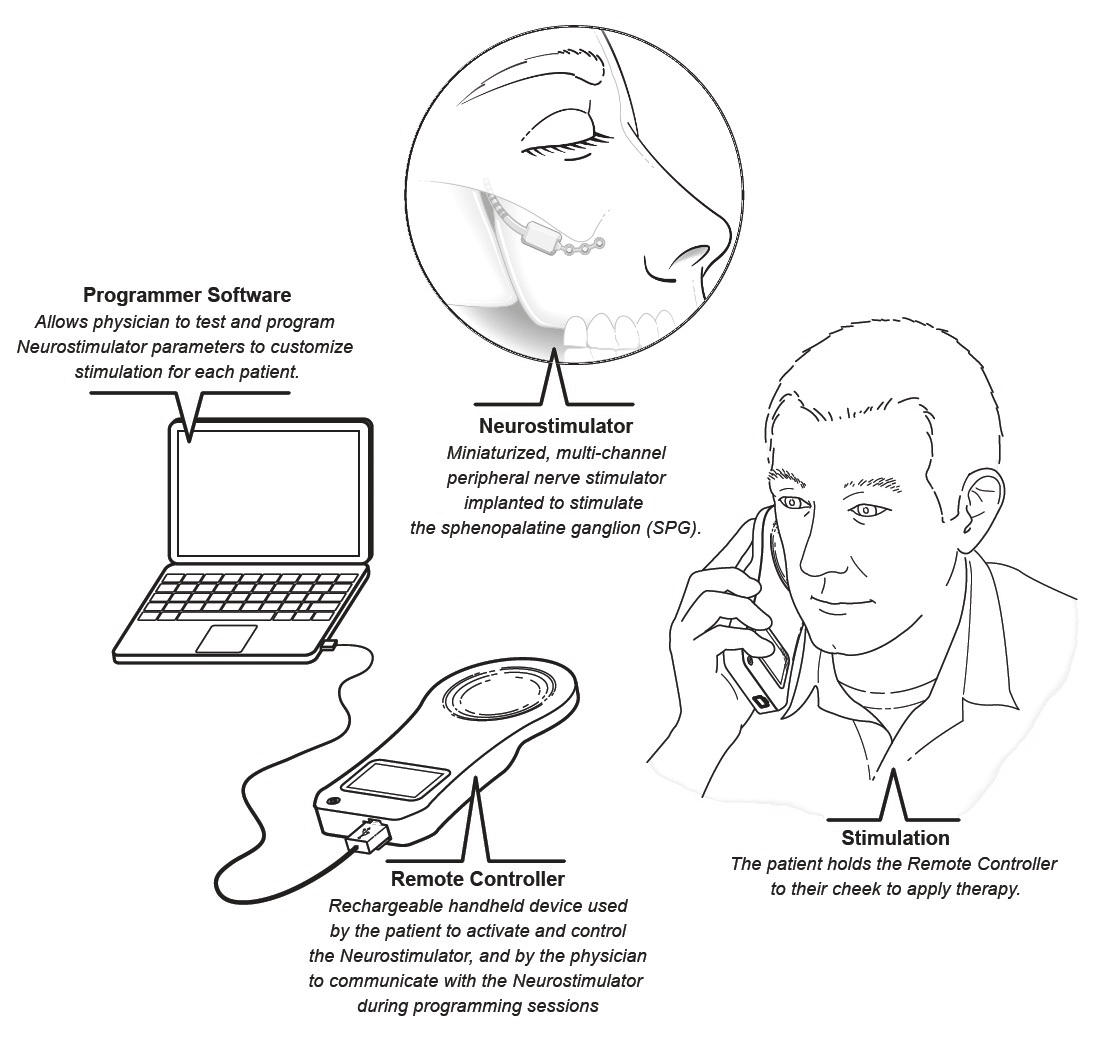
Head pain involves two big pathways. One’s the pain pathway that’s incoming and the other pathway is what’s called the cranial autonomic pathway and that goes through the sphenopalatine ganglion. That other pathway is the thing that expresses things like eye watering, eye redness, nasal stuffiness, ear congestion, eyelid swelling and drooping — they’re called cranial autonomic symptoms.
If you take any person, if you give them enough pain — if you inject chili pepper or acid into someone’s forehead — then they get pain and they get a little bit of those symptoms. You’ve seen it in Migraine, if you ask enough people, and indeed some of this is seen in the misdiagnosis of sinus headache.
In Cluster Headache1, it’s very prominent, this activation. Over the last 25 years, this anatomy and physiology has been sorted out, and that will show you that this sphenopalatine ganglion is the major mediator of this autonomic pathway. So it’s an important part of the Cluster story, if I could put it that way.
It’s been known for a while that you could fiddle around with the ganglion, put local anesthetic in there. People used to put cocaine in there — I don’t mean recreationally, but from a therapeutic perspective. The problem with all of that is blinding. That’s not surprising.
I think that there is a general direction in the primary headache disorders treatment toward neuromodulation. We want treatments that are modulatory and not destructive. So, if I turn the clock back 20 years, what would be done for Cluster would be burning the trigeminal ganglion with thermocoagulation or local anesthetic or local alcohol injections. Some patients would go and have the nerve itself sectioned through the posterior fossa process. Cutting, burning, and slashing nerves is not a good idea. As time’s gone on, I think everyone’s understood that.
Neuromodulation has come along to try and change the way the brain behaves, the way these pathways behave, without doing anything destructive. So the worst case, it doesn’t work. You take it out and walk away. You can’t put the nerve back together when you cut it. It’s really quite important. These developments — the big picture — mean that whatever gets done to people, if it’s wrong, at least it’s not permanent. Twenty-five years ago, if it was wrong, it was permanent.
Tammy Rome:
Cluster headache patients are willing to take that risk
Dr. Goadsby:
Well, yeah. The thing about Cluster patients is that they’re willing to have deep brain stimulation — drill a hole, put the electrodes in. The death rate from that’s low, but it’s death. You say it casually, but, obviously, death is a bad outcome. So, the Cluster patients will tell you, “Do whatever you need to do.”
Treatments have moved in this direction where “do whatever you need to do” gets in line with the first principle of medicine which is “first, do no harm.”
 Sphenopalatine physiology has been known — I’ve been working on it since the 1990s — and this structure’s important. Fast-forward, we can block it. The ATI2 folks developed a stimulator device.
Sphenopalatine physiology has been known — I’ve been working on it since the 1990s — and this structure’s important. Fast-forward, we can block it. The ATI2 folks developed a stimulator device.
Teri Robert:
We’ve seen that. It’s wonderful.
Dr. Goadsby:
Yeah, real cool. It’s about the size of a matchstick that’s placed up in something called the pyterogine palatine fossa. They go up through the top of the mouth, top of the gum and make a little incision and then literally push this thing in through the hole and then affix it to the jaws with some little screws. It’s a nice piece of work. It’s relatively easy to do. The procedure is 40-60 minutes. Most of it is in the preparation, making sure everything’s perfect.
Tammy Rome:
How does that compare to a dental surgery or neurostim implant in complication severity?
Dr. Goadsby:
That’s exactly the right question. The facial maxillary people say it’s like doing a slightly more complicated surgery for an impacted tooth or other dental procedure. What’s important is the preparation: dental hygiene beforehand, clean the mouth properly, clean things afterward — it’s all about the local things.
Certainly, what’s been reported, you don’t see anything more than what you’d expect if you start doing dental and facial maxillary procedures in the upper jaw. So, that’s all sort of pretty predictable. You can do very careful preparatory work with the software to see, to use CT, to look at the structure of the area before you go so you know where to angle it. It’s not done blind and not done generically, but you take the individual. You do the CT so you can take a look at their path and their bone and their structure and make measurements.
Tammy Rome:
They know what they’re getting into before they go in?
Dr. Goadsby:
…and know exactly where you want to go and what you’re getting into, and what’s going on. It’s not like one shoe has to fit all in the size of the procedure. You can quite individualize it for the individual and their anatomy and that’s a good thing. So, that’s how the implantation is done.
There have been two studies. The first study, the so-called CH-1 study published by John Sherman several years ago, was done in Europe.

The other thing about it is that the current’s induced, so the stimulator on the outside induces the current. Cluster folks who’ve have occipital nerve stimulation will know that eventually their batteries need replacing. This doesn’t have a battery. You literally buy a nine-volt battery, put it in and do the stimulation from the outside, so that’s helpful in itself.
It’s also enabled the design of the second study, to get around blinding. The gadget we use for control in the second study gives a cutaneous electrical sensations so people can’t tell whether they’ve got active or not, which is real important from a design perspective and very important from a regulator buying into it, understanding it was done properly, all that kind of thing, which is terribly important when people go to decide whether something should be licensed or not.
So, first study—the design and the idea has been to stop attacks. So, you get an attack, you put the thing on and end the attack. These were all done in chronic Cluster Headache, by the way. What we noticed in the first study is that it worked for attacks, but a good proportion (about a third) had their attacks stop. It made a complexity in the first study because if attacks stop you can’t measure the attacks anymore. From a design perspective, it’s irritating. From the patient perspective, not so much. The same thing has emerged from the second study.
What we’re going to see here presented is the CH-2 study, a bigger study done with this really good blinding. It works on pain-free and pain relief in 15 minutes and it works on attack frequency and with no new side effect problems—nothing that you wouldn’t predict from someone poking around in the upper jaw, so to speak. Obviously pain afterwards. Very often we see an attack triggered afterwards. It’s not surprising and we treat it. No cluster patient has said they minded getting an attack treated if their other attacks are gonna stop.
So, we see two sorts of responders: there’s the frequency again in the attack responder set, that is, it will control their attacks but doesn’t affect the frequency. Then there’s a group of people, a bigger group in fact, who have the frequency go down and there are some who get both.
It’s pretty good long-term data now on it. So that’s CH-2. That’s a second study, and a very well-designed study, I’d like to say, that will go to the regulatory people. I think we can expect the regulatory people to take a good view of it because it’s well-done and it’s safe and there’s been now, quite an extensive European experience in terms of the safety database. So, it’s all good news. It will be interesting to see how the FDA handles it. They’re pretty sensible about Cluster Headaches, so it should be fine.
There is the long-term data from the European experience. It’s pretty clear that most, meaning, nine out of 10 people who get a response at six months will still have it at 12 months or 18 months or two years
Tammy Rome:
So, it doesn’t diminish?
Dr. Goadsby:
No, it doesn’t diminish. Well, for nine out of 10 it doesn’t diminish. Nothing’s perfect. So, for the majority, the investment is looking like, not an investment of six months or 12 months or 18 months — you get this thing and then you get a response that’s going over much longer periods of time. I don’t know what’s going to happen in five years or 10 years, but when I think of patients with chronic Cluster Headache, if I told them I was going to do this thing and they’d have improvement for six months, they’d jump at it.
Tammy Rome:
We’ll take it.
Dr. Goadsby:
Exactly. If I told them it’s for almost two years, they’d just cry and say, “Go ahead. This afternoon would be fine, tomorrow if you have to delay.” So, I think it’s a really big development and it’s in the context that other things failed in chronic Cluster Headache. So, the CGRPs have failed. The Lily folks — the episodic worked, but the chronic didn’t. The Teva folks have pulled their chronic study for futility.
Tammy Rome:
I’ve had colleagues in tears because they were pulled from the trial.
Dr. Goadsby:
Exactly. But good to stop something that doesn’t work.
Tammy Rome:
It was a mixed feeling.
Dr. Goadsby:
Yeah, it’s a mixed feeling because you don’t want people suffering on a placebo for no particularly good purpose. If it’s failed for two of them, probably means it does fail. Then you’ve got the nVNS story. That seems to have failed. It’s not useful in acute attacks in chronic Cluster Headache. Now I kind of see this sphenopalatine thing as a bit of a beacon, a light on the hill, because if it wasn’t for that, chronic Cluster Headache people would finish this year with a kind of “well, everything failed,” and that would be pretty hopeless.
Tammy Rome:
They already feel pretty hopeless as it is.
Dr. Goadsby:
So far all the patients we’ve implanted in London have all had a response. One description or another would all say that it was great. I’ve got this one guy. I could cry. He told me he felt like he’d got the best Christmas present of his whole life. You just don’t know what to say when someone says that to you.
Tammy Rome:
After the device is implanted, what can patients expect in terms of recovery from the procedure?
Dr. Goadsby:
Yeah, the recovery from the procedure takes weeks. Have a tooth extraction, have a wisdom tooth extraction and put that a little beyond that. It takes weeks. I wouldn’t see any complications from that. It settles down pretty quickly — a little bit of local discomfort but that’s it. It can be a sense of numbness or tingling. That can take a little longer to settle down — a couple of months. The thing about chronic Cluster Headache patients is when you start talking about a bit of tingling and a bit of discomfort, they think it’s a joke.
Tammy Rome:
It is a joke.
Teri Robert:
Tammy has chronic Cluster Headache.
Dr. Goadsby:
Yeah, exactly. So I feel the need to say it, but I do understand that you kind of wonder why I bother.
Tammy Rome:
Tingling? Bring it on.
Dr. Goadsby:
Exactly, “Is that the best you can do? Is there something else?”
Tammy Rome:
Can patient’s start treating right away or do they have to wait?
Dr. Goadsby:
We give them a short break, a couple of weeks.
Tammy Rome:
If it’s going to work, how soon do they see results?
Dr. Goadsby:
About a fifth will see it in the first week, literally.
Tammy Rome:
That’s beautiful.
Dr. Goadsby:
Yeah, it’s extraordinary when they start seeing it that quickly. About a fifth will see it within a week to a couple of weeks. Then the larger group will certainly start to see their benefit within about six weeks. It builds up.
Tammy Rome:
…and that includes the acute response and the long-term preventive?
Dr. Goadsby:
That’s right.
Tammy Rome:
So how long do you wait before you say, “Okay, this isn’t working for me?”
Dr. Goadsby:
That’s an interesting question. I haven’t had anyone so far. I’ve been fortunate enough to work with a facial-maxillary surgeon and a skull-based neurosurgeon who are willing to be in the same room with each other. They’re good people. They’re really excellent and they understand how important this is. So I get them in there to get perfection because I expect them to get perfection. So we haven’t had anyone who hasn’t responded yet. I haven’t come across that problem.
My European colleagues tell me they will persist for at least six months to try. The electrodes — you can vary where you stimulate and the current that you put across it. So there’s a certain work of getting it right. I wouldn’t give up until six months.
You’ve got to be patient. Neuromodulation is neuromodulation and patience is really quite important. Your troops, they need to know about this work and watch very carefully what happens.
Tammy Rome:
We’ve been watching.
Dr. Goadsby:
And also, when it gets available, seek out people who’ve done it before. It’s not like brushing your teeth or having a dentist drill. The person who does it really well gets a really really good result. My view is that there’s less people doing more, getting really good at it, than every Tom, Dick, and Harry running around getting a shoddy job. A lot of my colleagues would kill me for saying this, but you’re the end point here. It seems perfectly clear that good operator gets a better result. Better to seek out someone who knows what they’re doing. Ask if they’ve done it before and what training they’ve had.
Tammy Rome:
So, once it’s available, how would patients go about finding these experienced physicians?
Dr. Goadsby:
It will probably be listed on their website. The physicians and surgeons who’ve been involved in the study will all be listed. It’s not a big secret because they’re going to be proud of themselves. Seek out the people who were involved in the study where it worked as opposed to people who just read on the internet. Better to wait for a really good result than get a poor result quickly.
Notes:
- Cluster Headache is a primary headache disorder characterized by frequent attacks of severe pain lasting 30 minutes to 3 hours. These attacks come in cycles (i.e. “clusters”) followed by pain free periods. Chronic Cluster Headache does not have pain-free periods. Attacks can occur once every other day or as frequently as eight times per day. Learn more at the Cluster Headache Support Group.
- ATI refers to Autonomic Technologies, Inc., the makers of the SPG microstimulator system referred to in this interview.